
Small cell lung cancer (SCLC) occurs almost exclusively in smokers and represents 15 to 25% of all lung cancer histologies and in bronchogenic carcinomas.At the time of diagnosis, approximately 30% of patients with SCLC will have tumors confined to the hemithorax of origin, the mediastinum, or the supraclavicular lymph nodes. It is distinguished from non-small cell lung cancer (NSCLC) by its rapid tumor doubling time, high growth fraction, and early development of widespread metastases. While SCLC is considered highly responsive to chemotherapy and radiotherapy, relapse despite treatment commonly occurs within 2 years.
 Overall, survival beyond 5 years occurs in 3 to 8% of patients with SCLC (7% with limited disease.
Overall, survival beyond 5 years occurs in 3 to 8% of patients with SCLC (7% with limited disease.
 other carcinogens over years. Multiple genetic defects are detected, some characteristic and perhaps involved with the process, and some random or secondary events. Included in the characteristic lesions is a loss of heterozygosity on chromosome 9p and deletion of 3p, including 3p21-22, leading to inactivation of as many as three putative tumor-suppressor genes. The identity of these genes is unknown, but several candidate regulatory genes reside in the vicinity (protein-tyrosine phosphatase-7, c-raf-1, p-retinoic acid receptor), none of which are felt to be the actual genes responsible. Loss of the retinoblastoma gene function at 13ql4 is ubiquitous. Approximately 60% of SCLC cell lines have undetectable transcripts, and the remaining 40% have an abnormal gene product. These abnormalities are also detected in fresh tumor specimens. p53 mutations are detected in most SCLC cell lines and fresh tumors.
other carcinogens over years. Multiple genetic defects are detected, some characteristic and perhaps involved with the process, and some random or secondary events. Included in the characteristic lesions is a loss of heterozygosity on chromosome 9p and deletion of 3p, including 3p21-22, leading to inactivation of as many as three putative tumor-suppressor genes. The identity of these genes is unknown, but several candidate regulatory genes reside in the vicinity (protein-tyrosine phosphatase-7, c-raf-1, p-retinoic acid receptor), none of which are felt to be the actual genes responsible. Loss of the retinoblastoma gene function at 13ql4 is ubiquitous. Approximately 60% of SCLC cell lines have undetectable transcripts, and the remaining 40% have an abnormal gene product. These abnormalities are also detected in fresh tumor specimens. p53 mutations are detected in most SCLC cell lines and fresh tumors.
Clinical Features
Lung cancer may present with symptoms or be found incidentally on chest imaging. Symptoms and signs may result from the location of the primary local invasion or compression of adjacent thoracic structures, distant metastases, or paraneoplastic phenomena. The most common symptoms at presentation are worsening cough, shortness of breath, and dyspnea.
Other presenting symptoms include the following:
Infrequently, patients with SCLC may present with symptoms and signs of one of the following paraneoplastic syndromes:
Diagnosis
Treatment options for patients are determined by histology, stage, and general health and comorbidities of the patient. Investigations of patients with suspected SCLC focus on confirming the diagnosis and determining the extent of the disease.
The procedures used to determine the presence of cancer include the following:
Staging Evaluation
Staging procedures for SCLC are important in distinguishing patients with disease limited to their thorax from those with distant metastases. At the time of initial diagnosis, approximately two-thirds of patients with SCLC have clinical evidence of metastases; most of the remaining patients have clinical evidence of extensive nodal involvement in the hilar, mediastinal, and sometimes supraclavicular regions.
Determining the stage of cancer allows an assessment of prognosis and a determination of treatment, particularly when chest radiation therapy or surgical excision is added to chemotherapy for patients with LD. If ED is confirmed, further evaluation should be individualized according to the signs and symptoms unique to the individual patient.
Standard staging procedures include the following:
The role of positron emission tomography (PET) is still under study. SCLC is fluorodeoxyglucose (FDG) avid at the primary site and at metastatic sites. PET may be used in staging patients with SCLC who are potential candidates for the addition of thoracic radiation therapy to chemotherapy, as PET may lead to upstaging or downstaging of patients and to alteration of radiation fields due to the identification of additional sites of nodal metastases.
Evidence (FDG-PET):
In a study of 120 patients with LD SCLC or ED SCLC, ten patients were upstaged and three patients were downstaged. PET was more sensitive and specific than CT scans for nonbrain distant metastases.
In a small series of 24 patients with LD by conventional staging, two patients were upstaged to ED. Unsuspected nodal metastases were documented in 25% of patients, which altered the radiation plan in these patients. At this time, sensitivity, specificity, and positive- or negative-predictive value of PET scanning and its enhancement of staging accuracy are uncertain.
Prognosis:
 physical examination, chest, liver, and adrenal CT scan,head MRI, bone scan and unilateral or bilateral bone marrow aspirates and biopsies. An alternate, abbreviated staging algorithm could be directed by symptoms and terminated with documentation of ED. This latter strategy, the rule for many European trials, is likely to become more prevalent in the United States in these times of health-care parsimony and need for economic justification. Specifically, many investigators argue that bone marrow examination, given the relative invasiveness of the procedure, has very low yield in patients with normal serum lactate dehydrogenase (LDH) levels. Arguments against sequential staging include the fact that bone scans
physical examination, chest, liver, and adrenal CT scan,head MRI, bone scan and unilateral or bilateral bone marrow aspirates and biopsies. An alternate, abbreviated staging algorithm could be directed by symptoms and terminated with documentation of ED. This latter strategy, the rule for many European trials, is likely to become more prevalent in the United States in these times of health-care parsimony and need for economic justification. Specifically, many investigators argue that bone marrow examination, given the relative invasiveness of the procedure, has very low yield in patients with normal serum lactate dehydrogenase (LDH) levels. Arguments against sequential staging include the fact that bone scans
Even after removes all the cancer that can be seen at the time of the operation, some patients may be given chemotherapy or radiation therapy after surgery to kill any cancer cells that are left. Treatment given after the surgery, to lower the risk that the cancer will come back, is called adjuvant therapy.
2) Chemotherapy
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy). When chemotherapy is placed directly into the cerebrospinal fluid, an organ, or a body cavity such as the abdomen, the drugs mainly affect cancer cells in those areas (regional chemotherapy). The way the chemotherapy is given depends on the type and stage of the cancer being treated.
Drugs Approved for Small Cell Lung Cancer includes
 5) Endoscopic stent placement
5) Endoscopic stent placement
 Overall, survival beyond 5 years occurs in 3 to 8% of patients with SCLC (7% with limited disease.
Overall, survival beyond 5 years occurs in 3 to 8% of patients with SCLC (7% with limited disease. Pathogensis
SCLC is characterized by small "blue" malignant cells about twice the size of lymphocytes, with sparse cytoplasmic and nuclear features having finely dispersed chromatin without distinct nucleoli. Nuclear molding is considered characteristic in well-preserved specimens, although a nondiagnostic "crush" artifact is more frequently observed. The histologic subtypes recognized in the pathology literature, classic oat cell and intermediate cell types,do not appear to behave differently biologically or clinically. On the other hand, histologic findings with combined large cell/small cell or mixed small cell with squamous cell or adenocarcinoma impart a poorer prognosis and greater resistance to treatment. While these histologic results are rarely detected in untreated specimens, the observation that up to 30% of autopsies demonstrate areas of NSCLC differentiation has led to the proposal that pulmonary carcinogenesis occurs in a pluripotent stem cell capable of differentiation along several pathways. Eight to 15 SCLC antigen clusters have been identified
by segregation analysis and divided into the following three groups: neural, epithelial, and neuroendocrine.
Epithelial differentiation is demonstrated by keratin expression. Neuroendocrine and neural differentiation result in the expression of dopa-decarboxylase, calcitonin, neurofilament, neural cell adhesion molecule, gastrin-releasing peptide, and insulin-like growth factor. Occasional hosts can produce antibodies (anti-r7w) that cross-react with both SCLC cells and the central nervous system and are associated width cerebral and cerebellar degenerative syndromes. Moreover, SCLC cells also produce a number of polypeptide hormones, including adrenocorticotrophic hormone and vasopressin, resulting in various paraneoplastic and ectopic hormonal syndromes. Insulin-like growth factor-1 and gastrin-releasing peptide may participate in autocrine and paracrine loops to enhance growth of SCLC cells. In addition to these growth factors being overexpressed, neural endopeptidase (common acute lymphoblastic leukemia antigen), the enzyme that inactivates these small polypeptide hormones, is underexpressed in SCLC cells and in bronchoalveolar lavage fluid from smokers.
The development of lung cancer occurs through mutagenesis and proliferative stimuli caused by tobacco and
 other carcinogens over years. Multiple genetic defects are detected, some characteristic and perhaps involved with the process, and some random or secondary events. Included in the characteristic lesions is a loss of heterozygosity on chromosome 9p and deletion of 3p, including 3p21-22, leading to inactivation of as many as three putative tumor-suppressor genes. The identity of these genes is unknown, but several candidate regulatory genes reside in the vicinity (protein-tyrosine phosphatase-7, c-raf-1, p-retinoic acid receptor), none of which are felt to be the actual genes responsible. Loss of the retinoblastoma gene function at 13ql4 is ubiquitous. Approximately 60% of SCLC cell lines have undetectable transcripts, and the remaining 40% have an abnormal gene product. These abnormalities are also detected in fresh tumor specimens. p53 mutations are detected in most SCLC cell lines and fresh tumors.
other carcinogens over years. Multiple genetic defects are detected, some characteristic and perhaps involved with the process, and some random or secondary events. Included in the characteristic lesions is a loss of heterozygosity on chromosome 9p and deletion of 3p, including 3p21-22, leading to inactivation of as many as three putative tumor-suppressor genes. The identity of these genes is unknown, but several candidate regulatory genes reside in the vicinity (protein-tyrosine phosphatase-7, c-raf-1, p-retinoic acid receptor), none of which are felt to be the actual genes responsible. Loss of the retinoblastoma gene function at 13ql4 is ubiquitous. Approximately 60% of SCLC cell lines have undetectable transcripts, and the remaining 40% have an abnormal gene product. These abnormalities are also detected in fresh tumor specimens. p53 mutations are detected in most SCLC cell lines and fresh tumors.Clinical Features
Lung cancer may present with symptoms or be found incidentally on chest imaging. Symptoms and signs may result from the location of the primary local invasion or compression of adjacent thoracic structures, distant metastases, or paraneoplastic phenomena. The most common symptoms at presentation are worsening cough, shortness of breath, and dyspnea.
Other presenting symptoms include the following:
- Chest pain.
- Hoarseness.
- Malaise.
- Anorexia.
- Weight loss.
- Hemoptysis.
Infrequently, patients with SCLC may present with symptoms and signs of one of the following paraneoplastic syndromes:
- Inappropriate antidiuretic hormone secretion.
- Cushing syndrome from secretion of adrenocorticotropic hormone.
- Paraneoplastic cerebellar degeneration.
- Lambert-Eaton myasthenic syndrome.
Diagnosis
Treatment options for patients are determined by histology, stage, and general health and comorbidities of the patient. Investigations of patients with suspected SCLC focus on confirming the diagnosis and determining the extent of the disease.
The procedures used to determine the presence of cancer include the following:
- History.
- Physical examination.
- Routine laboratory evaluations.
- Chest x-ray.
- Chest computed tomography scan with infusion of contrast material.
- Biopsy.
Staging Evaluation
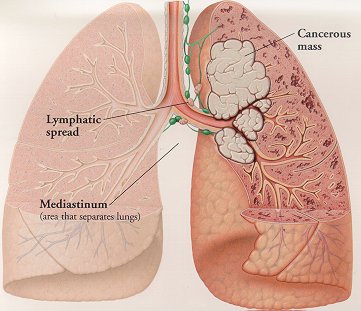
Staging procedures for SCLC are important in distinguishing patients with disease limited to their thorax from those with distant metastases. At the time of initial diagnosis, approximately two-thirds of patients with SCLC have clinical evidence of metastases; most of the remaining patients have clinical evidence of extensive nodal involvement in the hilar, mediastinal, and sometimes supraclavicular regions.
Determining the stage of cancer allows an assessment of prognosis and a determination of treatment, particularly when chest radiation therapy or surgical excision is added to chemotherapy for patients with LD. If ED is confirmed, further evaluation should be individualized according to the signs and symptoms unique to the individual patient.
Standard staging procedures include the following:
- A thorough physical examination.
- Routine blood counts and serum chemistries.
- Chest and upper abdominal computed tomography (CT) scanning.
- A radionuclide bone scan.
- A brain magnetic resonance imaging scan or CT scan.
The role of positron emission tomography (PET) is still under study. SCLC is fluorodeoxyglucose (FDG) avid at the primary site and at metastatic sites. PET may be used in staging patients with SCLC who are potential candidates for the addition of thoracic radiation therapy to chemotherapy, as PET may lead to upstaging or downstaging of patients and to alteration of radiation fields due to the identification of additional sites of nodal metastases.
Evidence (FDG-PET):
In a study of 120 patients with LD SCLC or ED SCLC, ten patients were upstaged and three patients were downstaged. PET was more sensitive and specific than CT scans for nonbrain distant metastases.
In a small series of 24 patients with LD by conventional staging, two patients were upstaged to ED. Unsuspected nodal metastases were documented in 25% of patients, which altered the radiation plan in these patients. At this time, sensitivity, specificity, and positive- or negative-predictive value of PET scanning and its enhancement of staging accuracy are uncertain.
Prognosis:
Systemic therapy is required for all patients with SCLC, even those with radiographically staged LD. Thus, the major therapeutic role of staging is to guide the use of chest radiotherapy, which is indicated for LD but not necessarily for ED. In addition to obtaining tissue diagnosis, exhaustive staging would include chest radiograph;
 physical examination, chest, liver, and adrenal CT scan,head MRI, bone scan and unilateral or bilateral bone marrow aspirates and biopsies. An alternate, abbreviated staging algorithm could be directed by symptoms and terminated with documentation of ED. This latter strategy, the rule for many European trials, is likely to become more prevalent in the United States in these times of health-care parsimony and need for economic justification. Specifically, many investigators argue that bone marrow examination, given the relative invasiveness of the procedure, has very low yield in patients with normal serum lactate dehydrogenase (LDH) levels. Arguments against sequential staging include the fact that bone scans
physical examination, chest, liver, and adrenal CT scan,head MRI, bone scan and unilateral or bilateral bone marrow aspirates and biopsies. An alternate, abbreviated staging algorithm could be directed by symptoms and terminated with documentation of ED. This latter strategy, the rule for many European trials, is likely to become more prevalent in the United States in these times of health-care parsimony and need for economic justification. Specifically, many investigators argue that bone marrow examination, given the relative invasiveness of the procedure, has very low yield in patients with normal serum lactate dehydrogenase (LDH) levels. Arguments against sequential staging include the fact that bone scansare positive in up to 30% of patients who do not have abnormal alkaline phosphatase levels or symptoms. A head CT scan is positive in about 15% of patients at diagnosis, one third of whom are asymptomatic, and early treatment of brain metastases yields a lower rate of chronic neurologic morbidity. Of greater importance is the swift progression of untreated SCLC. Most patients have developed their prediagnosis symptoms within the preceding weeks. Staging should not delay treatment more than 7 to10 days, or else many patients will become seriously ill.
The most important prognostic factors are performance status and body weight, as well as tumor-related factors involving extent of disease (LD vs ED). Within the LD subset, early stage disease (stage I) carries a favorable prognosis, whereas elevated LDH level indicates an unfavorable prognosis. Within the ED subset, the number of organ sites involved is inversely related to the prognosis.
Metastatic involvement of the central nervous system, bone marrow, or liver is unfavorable, compared with other sites, although these variables are confounded by the number of sites involved. The presence of paraneoplastic syndromes is also generally unfavorable.
Treatment:
Five types of standard treatment are used:
1) Surgery
Surgery may be used if the cancer is found in one lung and in nearby lymph nodes only. Because this type of lung cancer is usually found in both lungs, surgery alone is not often used. Occasionally, surgery may be used to help determine the patient’s exact type of lung cancer. During surgery, the doctor will also remove lymph nodes to see if they contain cancer.Even after removes all the cancer that can be seen at the time of the operation, some patients may be given chemotherapy or radiation therapy after surgery to kill any cancer cells that are left. Treatment given after the surgery, to lower the risk that the cancer will come back, is called adjuvant therapy.
2) Chemotherapy
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy). When chemotherapy is placed directly into the cerebrospinal fluid, an organ, or a body cavity such as the abdomen, the drugs mainly affect cancer cells in those areas (regional chemotherapy). The way the chemotherapy is given depends on the type and stage of the cancer being treated.
Drugs Approved for Small Cell Lung Cancer includes
- Methotrexate
- Etoposide
- Etoposide Phosphate
- Topotecan Hydrochloride
3) Radiation therapy
Radiation therapy is a cancer treatment that uses high-energy X-rays or other types of radiation to kill cancer cells or keep them from growing. There are two types of radiation therapy. External radiation therapy uses a machine outside the body to send radiation toward the cancer. Internal radiation therapy uses a radioactive substance sealed in needles, seeds, wires, or catheters that are placed directly into or near the cancer. Prophylactic cranial irradiation (radiation therapy to the brain to reduce the risk that cancer will spread to the brain) may also be given. The way the radiation therapy is given depends on the type and stage of the cancer being treated.
4)Laser therapy
Laser therapy is a cancer treatment that uses a laser beam (a narrow beam of intense light) to kill cancer cells.
5) Endoscopic stent placementAn endoscope is a thin, tube-like instrument used to look at tissues inside the body. An endoscope has a light and a lens for viewing and may be used to place a stent in a body structure to keep the structure open. Endoscopic stent placement can be used to open an airway blocked by abnormal tissue.
Smoking cessation:
The importance of quitting smoking cannot be overemphasized, particularly for patients with limited stage disease. Patients who continue to smoke do less well. One reason is that if they survive their first lung cancer, they have a substantial chance of developing a second lung cancer because of smoking. Furthermore, treatment with chemotherapy, radiation therapy, and surgery can cause lung damage. It is therefore important to have the best lung function possible prior to and after receiving treatment. Thus, if at all possible, patients should stop smoking.
This is also an important opportunity for family and friends to stop smoking. There are inherited genetic factors that increase the likelihood of getting lung cancer, especially if persons with these genetic factors smoke or are around those who do.
Thanking you
Akshaya Srikanth,
Pharm.D Internee
Tidak ada komentar:
Posting Komentar